- 4192 Devonwood Way, Ashburn, Virginia, 20148
- Helpline: +1 (703) 665-3747
The Dynamic Reciprocity Model: A Preliminary Framework for Understanding Early Caregiver- Offspring Interactions
- Home
- Back to Journal
- Article Details
Decades of literature support the long-term developmental and health consequences of early caregiver-offspring interactions [1]. However, a comprehensive model of these complex bidirectional relations that can be applied to typically and atypically developing infants/children and their caregivers is needed in order to extrapolate research findings to clinical settings across disciplines. Therefore, the following preliminary model links the World Health Organization’s (WHO) International Classification of Functioning, Disability and Health [2], theories of sensitive parenting [1], and dynamic systems theory [3, 4], drawing from empirical research literature from multiple professional fields including Psychology [5, 6], Physical Therapy [7, 8], Occupational Therapy [9, 10], and Speech-Language Pathology [11–13]. Figure 1 includes the following nine constructs of interest, many of which were derived from the WHO [2] ICF model, but have been modified in order to understand how infant-caregiver reciprocity may link other variables in the model:
- Biological / Genetic Factors: Physical, physiological, chemical, neurological, or epigenetic/genetic contributors to functioning and behavior.
- Health Status: Positive and negative indicators of health including behaviors that promote health and quality of life, healthcare access and effective utilization, and disease-specific markers. This includes mental and physical health, longevity, wellbeing, and social health.
- Body Functions & Structures: Physiological and psychological functions of the body, including mental, sensory/pain, voice/speech, movement, and major bodily system functions (i.e., cardiovascular, hematological, immunological, respiratory, digestive, metabolic, endocrine, genitourinary, reproductive, neuromuscular, and integumentary/exocrine system; WHO, 2001). Structures of the body include parts within the major anatomical systems that may hinder or facilitate bodily functioning [2].
- Goal-Directed Action: Execution of goal or task-oriented action or behavior by an individual, which may include purposeful sensory experiences, learning, knowledge application, completion of general everyday tasks, mobility, and self-care.
- Participation: Engagement or involvement in life situations or occupations to accomplish a perceived role, which may include communication, interpersonal interactions, participation in relationships, and completion of tasks or actions required to engage in educational, work/employment, economic transactions, community, social, and civic life [2].
- Reciprocity Behavior: Mutual, dyadic engagement, involving bidirectional temporal symmetry in actions and psychological states (Feldman, 2007). Reciprocity bridges gaps between internal and external factors in the model and serves as a mechanism to influence development.
- Environmental Factors: The larger physical, social, and attitudinal context where people live, which includes products, equipment, technology, the natural and human-adjusted environment, supportive and relationship factors, attitudes, services, systems, and policies [2]. With regard to reciprocity, the environment that the caregiver provides to or engages in with offspring.
- Personal Factors: One’s personal background, which is made up of sociodemographic aspects of the self, history, lifestyles/habits, and psychosocial variables [2]. With regard to reciprocity, caregiver-offspring interactions that are influenced by the above-mentioned personal factors.
- Contextual Factors: The foundation for environmental and personal factors, including cultural factors [2].
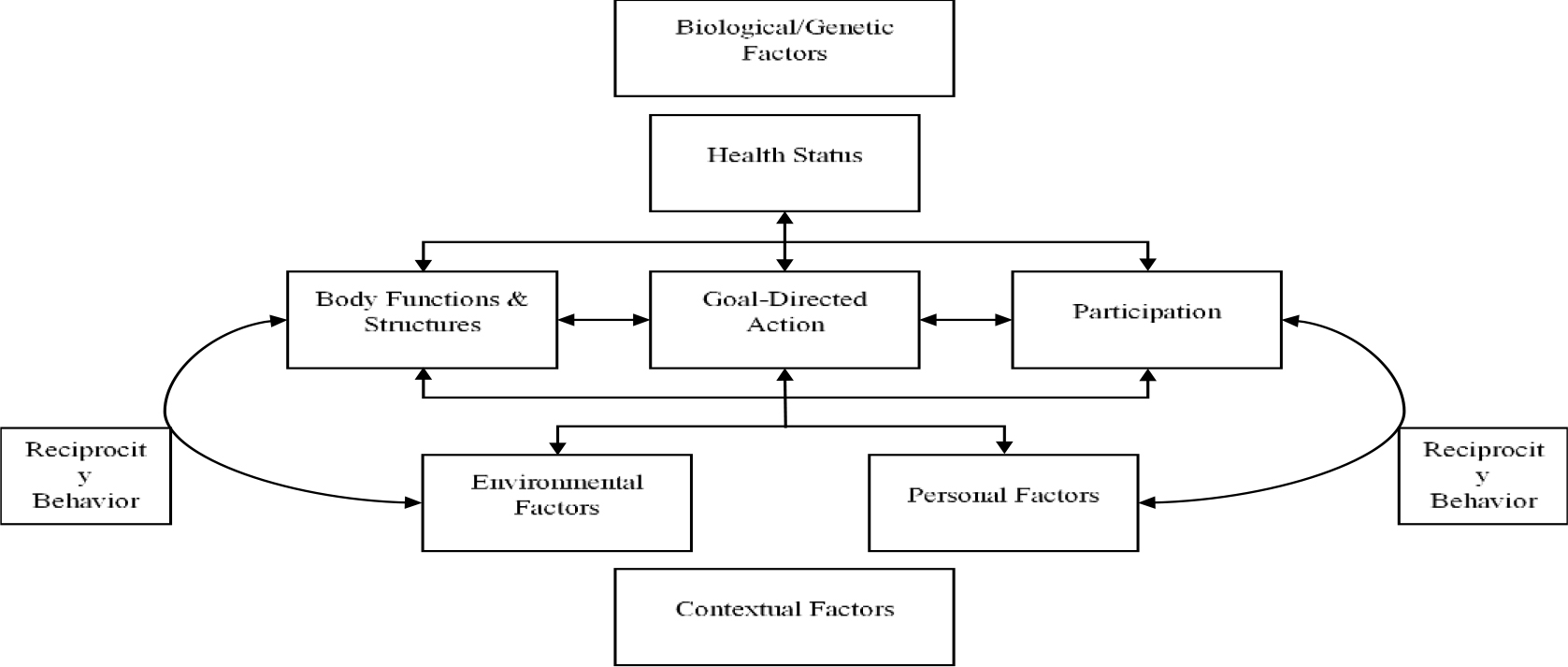
Figure 1. Dynamic Reciprocity Model. The model highlights how caregiver-offspring reciprocity interacts with other risk or resiliency factors to influence developmental and health outcomes.
Taken together, utilization of the above model of biopsychosocial factors may assist multidisciplinary researchers and clinicians in better communicating and understanding mechanisms and pathways that link caregiver-infant/child reciprocity and infant/child development. This may assist in informing prevention and intervention research to develop reciprocity-focused behavioral targets to improve child development and health across the lifespan. In particular, the above model represents work from collaborators in the fields of Psychology, Physical Therapy, Occupational Therapy, and Speech-Language Pathology, with unique practical implications in early educational, assessment, intervention, and rehabilitation settings.
References
- Leclère C, Viaux S, Avril M, Achard C, Chetouani M, et al. (2014) Why synchrony matters during mother-child interactions: a systematic review. PloS one 9: e113571. [View]
- World Health Organization. (2001) International classification of functioning, disability and health: ICF. World Health Organization. https://www.who.int/classifications/icf/en/
- Sweeney JK, Heriza CB, Blanchard Y, Dusing SC (2010) Neonatal physical therapy. Part II: Practice frameworks and evidence-based practice guidelines. Pediatric Physical Therapy 22: 2–16. [View]
- Ulrich BD (2010) Opportunities for early intervention based on theory, basic neuroscience, and clinical science. Physical Therapy 90: 1868–1880. [View]
- Feldman R (2007) Parent–infant synchrony and the construction of shared timing; physiological precursors, developmental outcomes, and risk conditions. Journal of Child Psychology and Psychiatry 48, 329–354. [View]
- Provenzi L, Scotto di Minico G, Giusti L, Guida E, Müller M (2018). Disentangling the dyadic dance: Theoretical, methodological and outcomes systematic review of mother-infant dyadic processes. Frontiers in Psychology 9: 348. [View]
- Dusing SC, Izzo T, Thacker LR, Galloway JC (2014) Postural complexity influences development in infants born preterm with brain injury: relating Perception-Action Theory to 3 cases. Physical Therapy, 94: 1508–1516. [View]
- Westcott SL, Burtner P (2004) Postural control in children: implications for pediatric practice. Physical & Occupational Therapy in Pediatrics 24: 5–55. [View]
- Dunn W (2007) Supporting children to participate successfully in everyday life by using sensory processing knowledge. Infants & Young Children 20: 84–101.
- Pizur-Barnekow K, Kamp K, Cashin S (2014) An investigation of maternal play styles during the co-occupation of maternal-infant play. Journal of Occupational Science 21: 202–209.
- Hirsh-Pasek K, Adamson LB, Bakeman R, Owen MT, Golinkoff RM, et al. (2015) The contribution of early communication quality to low-income children’s language success. Psychological Science 26: 1071–1083. [View]
- Rowe ML (2008) Child-directed speech: Relation to socioeconomic status, knowledge of child development and child vocabulary skill. Journal of Child Language 35: 185–205. [View]
- Tomasello M, Farrar MJ (1986) Joint attention and early language. Child Development 57: 1454–1463. [View]