- 4192 Devonwood Way, Ashburn, Virginia, 20148
- Helpline: +1 (703) 665-3747
Pattern of Early Presentation in the Emergency Department and Elective Level of Care for Suspected Coronavirus Disease (COVID-19): A Proposal by the Italian SIMEU Research & Study Group
- Home
- Back to Journal
- Article Details
Summary
No guidelines are published on disposition of patients with coronavirus disease (COVID-19) infection at arrival in the Emergency Department (ED); the initial symptoms of upper respiratory-tract infection, although apparently mild, may deteriorate – sometimes very rapidly – to respiratory distress syndrome with unfavorable outcome. A set of variables may be useful to predict deterioration in relation to the clinical pattern at presentation.
On the basis of the experience of emergency physicians involved in the Italian outbreak, we identified four clinical risk profiles at ED presentation, requiring different levels of care. Patients were graded on: a) responsiveness of respiratory impairment to oxygen delivery, measured by PaO2/FO2% categories; b) pattern of pulmonary damage at imaging; c) biochemical markers of organ injury. These clinical profiles correspond to four different dispositions: discharge after short ED evaluation, admission to ordinary wards, admission to intermediate care, admission to intensive care unit. In an overcrowded ED, the present proposal provides a frame to dictate solutions even with limited use of resources (e.g., Echo ultrasound instead of high-resolution computed tomography – HRCT). A prospective collection of hospital records is recommended to test the validity and the accuracy of the classification in predicting outcomes.
Keywords: Coronavirus disease, early presentation, level of care, emergency department.
Letter
Dear Sir,
The initial symptoms of coronavirus disease (COVID-19) frequently mimic mild upper respiratory-tract infection, but this presentation may worsen – sometimes very rapidly – to respiratory distress syndrome and unfavorable outcome [1]. From the perspective of physicians operating in Emergency Departments (ED), a prediction tool at initial assessment would be useful to risk-stratify patients for treatment selection. In a retrospective study, older age, high Sequential Organ Failure Assessment (SOFA) score and elevated D-dimer at admission have been selected as death predictors [2].
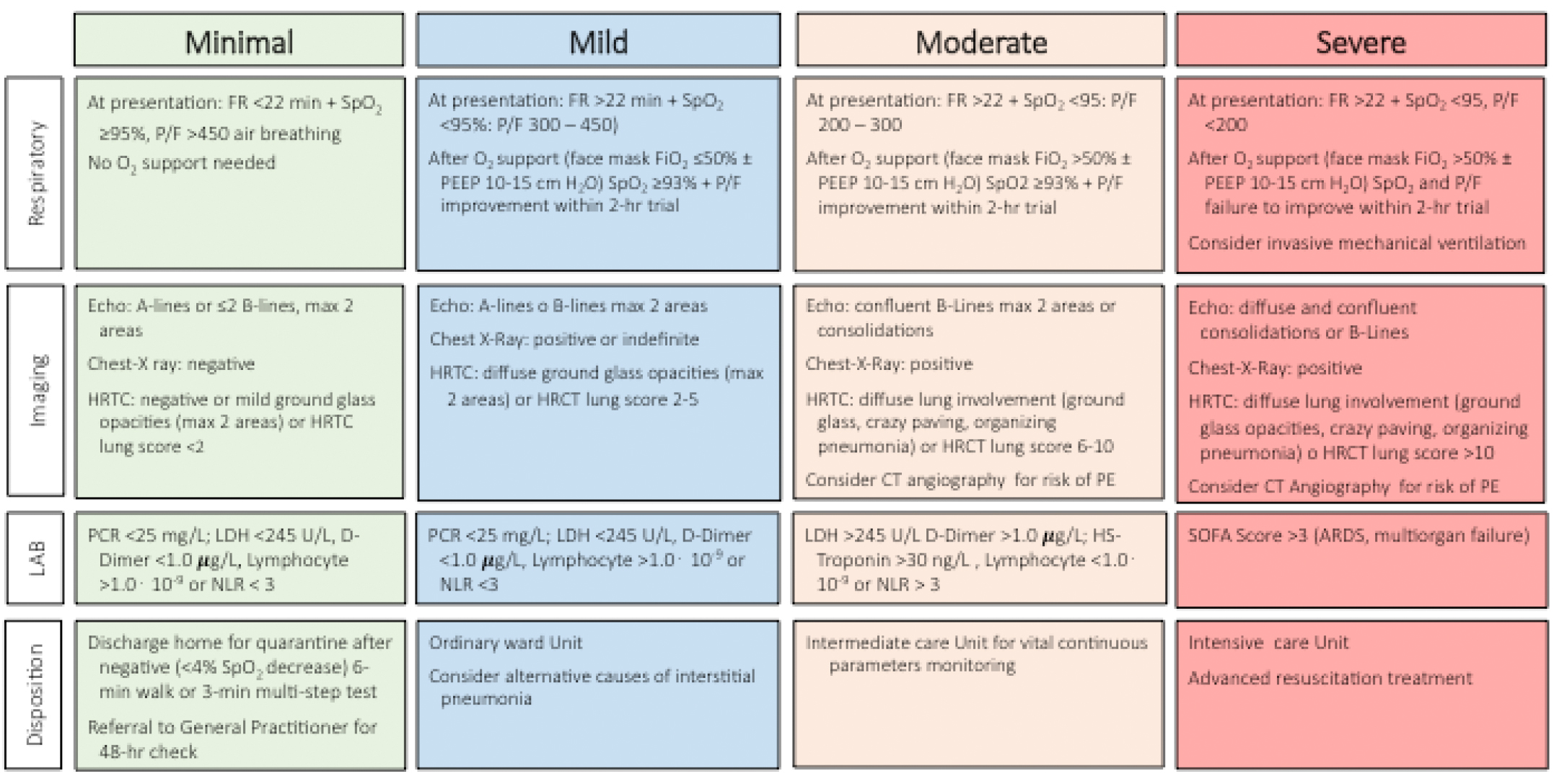
Based on empirical observations of health professionals, involved with hundreds of COVID cases in Italy, four clinical profiles may be identified at ED presentation, corresponding to increasing risks of complications and requiring different levels of care. Clinical profiles are defined by four different responses of respiratory impairment to oxygen delivery, measured by PaO2/FO2% ratio categories [3], by grading and pattern of pulmonary damage at imaging, and by biochemical markers of organ injury. These categories correspond to four different dispositions following ED arrival and eventually admission to hospital wards with increasing levels of care (Figure 1). In an overcrowded ED, the present proposal provides a frame to dictate solutions even with limited use of resources (e.g., lung ultrasonography instead of high-resolution computed tomography – HRCT).
Respiratory function: Respiratory function is measured by the analysis of blood gases at rest in breezing air at presentation and, in suspected cases, saturation during effort. At arrival, responders to a short trial with oxygen therapy by face mask (FiO2 ≤50%) require a different level of care compared with those who do not respond to regular oxygen support or to higher oxygen concentration support (CPAP, FiO2 >50%), eventually requiring mechanical ventilation also in the absence of altered vital parameters.
Chest Imaging: Chest X-ray [4], HRCT [5] or lung ultrasonography [6]. May be used to assess lung involvement, and a validated radiological score (HRCT Lung Score) [7], already used in SARS outbreak, has been re-proposed. The score correlates with the evolution of disease; it is based on rating 0–4 the percent involvement the five main lung districts. In high-risk subjects a computed tomographic pulmonary angiography must be considered in order to exclude/confirm pulmonary embolism [8].
Blood tests: A few blood tests are predictive of worsening disease, in particular LDH, PCR, D-Dimer, Troponin, and number of peripheral lymphocytes. Levels outside the normal limits should be considered as suggestive of unfavorable outcome.
Disposition: Following the comprehensive evaluation, the disposition should consider divergent levels of care, in relation to disease severity, in order to optimize hospital resources, reserving admission to intensive care units only to most severe cases.
The items discussed above are classified according to the following four risk classes:
Minimal Risk: It includes patients attending ED with a respiratory rate (RR) <22 breaths/min, arterial oxygenation (SpO2) >95% in room air and PaO2/FiO2 index (P/F) >450. SpO2 under effort (6-min walk test or 3-minute step test) is limited to less than 4%. No comorbidities or other risk factors are present (no cardiovascular diseases, diabetes mellitus, renal failure, chronic respiratory diseases, obesity, immunodepression, neoplasms, malnutrition, liver diseases, smoking or pregnancy) and age is <70. The lung parenchyma at imaging is normal or mildly impaired (ground glass lesions in <2 lung areas or HRCT score ≤2). Laboratory findings are normal.
These patients will undergo nasopharyngeal swabs before discharged, to be followed under fiduciary quarantine by GPs, who will be responsible for any therapy, with follow up by community services.
Mild Risk: These patients present with a RR >22 breath/min, SpO2 <95% in room air, and P/F ratio between 300 and 450. Usually several comorbidities or other risk factors are present (very frequently old age). They will be considered in the mild risk category if they respond to a 1- to 2-hour trial with facemask FiO2 ≤50% (criteria of response: SpO2 93–96%, improvement of P/F ratio following oxygen therapy). Chest X-ray is not always diagnostic; alternatively, HRCT or lung ultrasonography may show more than 2 lung areas involved, whereas HRCT lung score is 2–5. These patients need admission to ordinary ward for close surveillance and treatment. Monitoring will consist of regular control of arterial pressure, Glasgow Coma Scale, RR and SpO2 and a frequent check of blood gases (a significant drop of SpO2 is reported rather frequently).
Moderate Risk: These patients are characterized by RR >22, SpO2 <95, and P/F ratio between 200 and 300 at arrival. They will respond to 1- to 2-hour O2 support only by CPAP (PEEP 10–15) and FiO2 >50%, to a SpO2 value of 93–96, with P/F ratio improvement. Chest X-ray is always positive. Lung ultrasound shows confluent B-lines >2 lung areas or the presence of consolidation. HRCT shows diffuse lung involvement (ground glass opacities, crazy paving, organizing pneumonia) and the HRCT Lung Score is 6–10. Computed tomographic pulmonary angiography might be considered for suspect of pulmonary embolism [8]. The appropriate setting of care is an intermediate care unit, with continuous vital monitoring of vital signs (ECG, systolic blood pressure, GCS, RR, SpO2, PaO2 / FO2% ratio); SOFA score calculation and lactate measurement could help highlight early signs of shock.
Severe Risk: Patients at high risk of unfavorable outcome are characterized by FR >22, SatO2 <95% and P/F ratio <200 at presentation. SpO2 persists insufficient (<94%) and P/F does not improve despite a 1- to 2-hour O2 support with CPAP/NIV (PEEP 10–15) and FiO2 >50%. Chest X rays and lung ultrasound show confluent, diffuse consolidation and B-lines. HRCT shows diffuse ground glass opacities, crazy paving and consolidation. HRCT score is >10. In these subjects, transfer to Intensive Care Units needs to be immediately considered for early mechanical ventilation also in the absence of altered state of consciousness.
This risk stratification is based on consensus between experts; SIMEU supports an extensive, prospective collection of patients’ records according to present grading in order to test its validity and accuracy in the real-world. Considering the lack of validated guidelines on appropriate levels of care, this might be an initial effort to classify patients, allowing for better understanding of disease severity, treatment effects and final outcomes.
References
- Salzberger B, Gluck T, Ehrenstein B (2020) Successful containment of COVID-19: the WHO-Report on the COVID-19 outbreak in China. Infection 48: 151–153. [View]
- Wang D, Hu B, Hu C, Zhu F, Liu X, et al. (2020) Clinical characteristics of 138 hospitalized patients with 2019 novel coronavirus-infected pneumonia in Wuhan, China. JAMA 323: 1061–1069. [View]
- Force ADT, Ranieri VM, Rubenfeld GD, Thompson BT, Ferguson ND, et al. (2012) Acute respiratory distress syndrome: the Berlin Definition. JAMA 307: 2526–2533. [View]
- Ai T, Yang Z, Hou H, Zhan C, Chen C, et al. (2020) Correlation of chest CT and RT-PCR testing in coronavirus disease 2019 (COVID-19) in China: A report of 1014 cases. Radiology 296: 200642. [View]
- Liu KC, Xu P, Lv WF, Qiu XH, Yao JL, et al. (2020) CT manifestations of coronavirus disease-2019: A retrospective analysis of 73 cases by disease severity. Eur J Radiol 126: 108941. [View]
- Peng QY, Wang XT, Zhang LN, Chinese Critical Care Ultrasound Study G (2020) Findings of lung ultrasonography of novel corona virus pneumonia during the 2019–2020epidemic. Intensive Care Med. 46: 849–850. [View]
- Li K, Fang Y, Li W, Pan C, Qin P, et al. (2020) CT image visual quantitative evaluation and clinical classification of coronavirus disease (COVID-19). Eur Radiol 30: 4407–4416. [View]
- Danzi GB, Loffi M, Galeazzi G, Gherbesi E (2020) Acute pulmonary embolism and COVID-19 pneumonia: a random association? Eur Heart J 41: 858. [View]