- 4192 Devonwood Way, Ashburn, Virginia, 20148
- Helpline: +1 (703) 665-3747
Embryonic Rhabdomyosarcoma of the Nasopharynx: a Case Report and Literature Review
- Home
- Back to Journal
- Article Details
Embryonal Rhabdomyosarcoma (ERMS) is a rare soft-tissue malignant tumor that occurs mostly in the skeletal muscles of the trunk, limbs, etc., and can also occur in tissues and organs lacking skeletal muscle. However, ERMS occurs in the nasopharynx less See [1], due to the lack of early clinical features, it is easy to be misdiagnosed or missed. With the development of comprehensive treatment models, its prognosis is better than that of acinar and undifferentiated rhabdomyosarcoma [2].
Keywords: Nasopharyngeal tumor; Rhabdomyosarcoma; Case report
Clinical Data
Clinical Manifestation
The clinical data of a patient with this disease recently admitted to our hospital are now reviewed and the literature review report is as follows. Patient, male, 22 years old, with progressive right nasal obstruction and right neck mass for 1+ month, left neck mass was admitted to our hospital on November 1, 2011. The patient had no obvious inducement in September 2011 Right nasal obstruction, no runny nose and hemorrhagic blood, and found a right neck mass, about 2X2cm 2 in size, without pain and tenderness. In the past 1+ months, the patient’s right nasal obstruction has progressively increased and the right neck mass has rapidly increased. Grow up. In the middle of October 2011, he began to have right eye tears without obvious visual changes. At the end of October 2011, the patient found a left neck mass without pain, fever, hoarseness and other discomforts. He was admitted to our hospital’s Otorhinolaryngology Head and Neck Surgery After perfecting the relevant examination, considering the wide range of lesions, it is difficult to completely remove the tumor during surgery, and then transferred to our department. Physical examination: weight kg, height cm, body surface area m 2, KPS 90 points. Right submandibular, sternocele the upper part of the processus muscle can be combined with multiple hard masses, fused into a mass, about 14* 12cm, fixed, unclear borders, no tenderness, no ulceration and swelling on the surface. Right upper clavicle fossa, left sternocleidomastoid mastoid the upper part of the muscle can be palpable with hard mass, the border is unclear, fixed, and there is no tenderness. There is no abnormality in the heart, lungs and abdomen.
Auxiliary Inspection
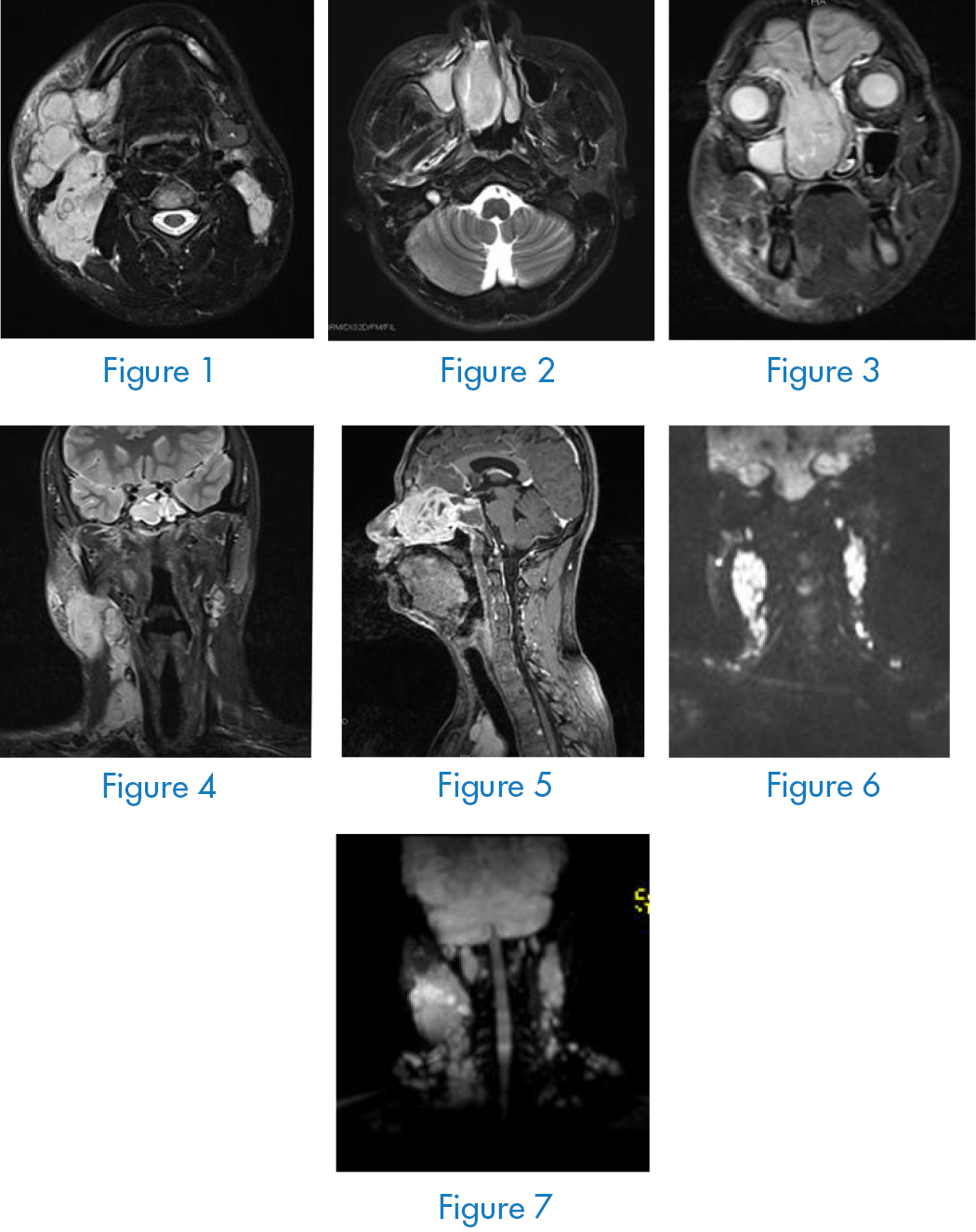
Nasopharyngeal neck enhancement MRI (Figure 1–7): the right nasal cavity involves abnormal signal masses of the ethmoid sinus, maxillary sinus, and frontal sinus and is significantly unevenly strengthened, which is consistent with the performance of embryonal rhabdomyosarcoma, and the bone of the inner side wall of the right maxillary sinus Damage, right frontal base may be involved, multiple lymph node metastases in the right pharyngeal side, submandibular area, bilateral deep neck, carotid sheath area, right frontal sinus, sphenoid sinus, and maxillary sinus with effusion. Head MRI, thoracoabdominal CT No abnormalities were found in bone scans. A new biopsy of the right nasal cavity was performed, and the pathological diagnosis was: (right nasal cavity) embryonic rhabdomyosarcoma. Immunohistochemistry: Final diagnosis: right nasal embryonic rhabdomyosarcoma phase III [3].
Treatment Methods and Effects
The patient had a large mass and rapid growth, and first underwent CVAD chemotherapy [3], [4], specifically: cyclophosphamide (CTX) 800mg / m 2 d 1, vincristine (VCR) 1.0mg / m 2 d 1, Epirubicin (EPI) 70mg / m 2 d 1, Azamidamide (DTIC) 100mg / m 2 d 1–5. Every 21 days is a cycle, a total of 2 cycles. At the same time, cervical lymph nodes were treated with TF36 (recombinant human p53 adenovirus injection) 2 × 10 12 intratumoral gene targeted therapy. Review of nasopharyngeal neck enhancement CT after 1 cycle of chemotherapy and targeted therapy (Figure 7) shows: after chemotherapy, local radiotherapy for bilateral cervical lymph nodes was arranged, with a total dose of 55 Gy. The patient is currently being followed up.
Discussion
The author reviews the literature related to ERMS and the cases reported in the past 5 years. The following discusses its clinical pathological characteristics, treatment and prognosis.
Pathological Characteristics
Rhabdomyosarcoma (RMS) is a highly malignant soft tissue tumor that originates from embryonic mesenchymal cells [5] with striated muscle differentiation potential. It can occur in any part of the body, where the RMS without striated muscle organs is much more frequent than the striated muscle itself High, because the pluripotent primitive mesenchymal tissue metaplasia is striated muscle cells or early striated myoblasts ectopic to abnormal sites with deformities [6]. According to the clinical characteristics, morphology, degree of differentiation of tumor cells and special tissue structure this disease can be divided into five types: grape cluster type, spindle cell type, embryo type, acinar type and polymorphic type [7]. Different tissue types are closely related to the age and location of onset. ERMS is common the subtype, which accounts for more than 50% to 60%, is derived from pluripotent embryonic cells, immature potential muscle tissue or undifferentiated mesoderm cells that will differentiate into muscle fibers. This type is related to fetuses at 7 to 12 weeks of pregnancy. The degree of development of skeletal muscle is very similar [3]. Under light microscopy, ERMS shows more undifferentiated mesenchymal cells, focal mucus-like changes, spindle cells or small round cells with obvious eosinophilic cytoplasm, and special Textured Cells [8]. In the case of poorly differentiated or undifferentiated, immunohistochemical staining is needed to further confirm the diagnosis. Its immunohistochemical markers mainly include myoglobin, myogenic determinant 1 (MyoD1), and skeletal myosin (desmin), muscle-specific actin, myogenin, etc.
Clinical Characteristics
Early symptoms are usually not obvious, showing only nasal congestion, runny nose, nausea, headache and other discomforts. When local symptoms or lumps appear, the disease is already advanced. ERMS occur in the head and neck, retroperitoneum and urogenital system, and ERMS in the nasal cavity and sinuses are very rare [1]. They mostly occur in children <15 years old and infants, while adults >40 years are very rare. The maximum reported age of onset is 72 years [9]. The main characteristics are malignancy, rapid progress, and early invasion of adjacent tissues, early lymph nodes and blood channel metastasis [1]. Due to its cryptic growth, early detection of tumors is very difficult, and the special anatomical structure of the ear, nose, and throat makes it difficult to completely remove the tumor tissue. At the time, CT and MRI applications are very necessary, they help to define the extent of the lesion and the degree of infiltration around it, and can be used as an important basis for localization diagnosis and selection of surgical methods [10]. Therefore, early detection and early diagnosis can improve the surgical resection rate and prolong Patient survival is important.
Treatment and Prognosis
ERMS has a high degree of malignancy, invasive growth, high recurrence rate, and the prognosis is not optimistic. With the development of radiotherapy and chemotherapy, molecular targeting, gene targeted therapy, and the progress made in the treatment of this disease, at present, the treatment of ERMS Multidisciplinary comprehensive treatment methods such as surgery, chemotherapy, radiotherapy, and targeted therapy are mostly used.
Because of the complexity of nasal anatomy and the easy transfer of RMS of the nasal cavity and sinuses into the skull, radical surgery is very difficult [11]. But as much tumor resection as possible is a guarantee of successful treatment. With the development of surgical technology, surgical experience Accumulation and application of intraoperative image navigation system have been able to remove most of the tumors of the head and neck, skull base and nasal-sinus area, ensure the safety of the resection margin, and reduce the recurrence rate [12]. Wurm J and other studies analyzed 15 cases of the nose for patients with ERMS, the results show that the 5-year survival rate (66%) in the surgery plus radio-chemotherapy group is significantly improved [13] compared to the 5-year survival rate (33%) in the radio-chemotherapy group alone. The range of surgical resection is based on the incidence of tumors Depending on the location; size, and clinical stage, cervical metastatic lymph nodes with clinical suspicion should undergo surgical biopsy or regional dissection. According to the staging criteria of the 1988 rhabdomyosarcoma study group [3], the disease can be divided into 4 stages: stage I It is localized, that is, the localized tumor can be completely resected, and regional lymph nodes are not invaded; stage II is regional, that is, localized infiltration of the tumor, invades surrounding tissues or regional lymph nodes; stage III is extensive, that is, it cannot be completely removed or only Biopsy with gross eyes Residues; IV period have distant metastases at diagnosis for I,II patients should be performed as radical surgery, III of patients with chemotherapy before surgery or cytoreductive surgery feasible, IV stage has lost the chance of operation.
Based on the biological characteristics of soft tissue sarcoma, systemic chemotherapy and high-dose radiotherapy can relatively prolong the survival of patients. The choice of chemotherapy regimen and the duration of treatment are closely related to the improvement of patient survival. The dose of the drug should be based on the patient’s condition, age, and tolerance. Applicable as appropriate. For patients with distant metastases, there are reports in the literature that increasing the dose does not improve the patient’s prognosis [14]. The current commonly used chemotherapy regimens are: VAC (VCR + actinomycin D + CTX), VCA (VCR + radiotherapy Dactycin D + CTX + Doxorubicin), CVAD (CTX + VCR + EPI + DTIC) [3], [4]. For patients who cannot undergo surgical resection and cannot tolerate systemic chemotherapy, superficial temporal artery intubation chemotherapy can be considered. Increasing the drug concentration in the tumor to obtain the therapeutic effect [15]. Accelerators are often used for radiotherapy, and the dose depends on the age. The total dose is generally 45~ 60Gy, and the course of treatment is 5 ~ 6 weeks. It is also reported that when using a dose of 65 ~ 75Gy It can increase the local control rate of RMS [16]. It is recommended that cervical lymphatic drainage area can be prophylactically irradiated at a dose of 50 ~ 60Gy [3].
In the past 20 years, research on the pathogenesis of RMS and cellular mechanisms and pathways related to survival rates, such as the RTK family, cell cycle regulatory white-dependent kinase inhibitors, insulin-like growth factor pathways, mammalian rapamycin target pathways, etc. It provides a new idea for molecular targeted therapy of RMS [17]. For gene therapy, the current application of recombinant human p53 adenovirus injection has a better effect on improving the short-term efficacy and survival rate of patients [7], [18], and Fewer side effects, safe and effective [19].
In summary, the combination of surgery-based and radiotherapy and chemotherapy-based targeted therapy is the key to improving the survival rate and quality of life of patients. Its prognosis and tumorigenesis location, size, clinical stage, whether surgery and other factors Related. Although there are many new developments in treatment methods, combined with domestic and foreign literature reports, the current overall treatment effect of adult head and neck RMS is poor, and the 5-year survival rate is about 8% [20]. Thankfully, Tsung -Han Wu and others recently published two case reports of ERMS with long-term survival rates of 12 and 19 years [4].
Acknowledgement
This project is funded by the research and data on the evaluation method of ster tactic radiotherapy equipment (subject no. : 2017YFC0113701).
References
- Yu Xiaoping, Liang Zhaoyu, Wang Ping (2006) Imaging manifestations of rhabdomyosarcoma in adults [J]. Journal of Clinical Radiology 25: 612–615.
- Moretti G, Guimarães R, Oliveira KM, Sanjar F, Voegels RL (2010) Rhabdomyosarcoma of the head and neck: 24 cases and literature review. Braz J Otorhinolaryngol 76: 533–537. [View]
- Wu Xin, Li Ping, Xie Li (2008) Clinical analysis of 13 cases of rhabdomyosarcoma of the nasal embryo type [j]. Journal of Clinical Otorhinolaryngology Head and Neck Surgery 22: 338–341. [View]
- Wu TH, Huang JS, Wang HM, Wang CH, Yeh KY (2010) Long-term Survivors of Adult Rhabdomyosarcoma of Maxillary Sinus Following Multimodal Therapy: Case Reports and Literature Reviews [J]. Chang Gung Med J 33: 466–470. [View]
- Gu Milli, Yin Weibo, Yu Zihao, et al. (2009) Radiation Oncology (Fourth Edition), China Union Medical College Press, 2009: 1278.
- Daya H, Chan HS, Sirkin W (2000) Pediatric rhabdomvosarcoma of the head and neck: is there a place for SurgicaI managemenet[J]. Arch 0tolaryllgol Head Neck Surg 126: 468–472.
- Peng Z (2005) Current status of gendicine in China: recombinant human Ad-p53 agent for treatment of cancers. Hum Gene Ther 16: 1016–1027. [View]
- Mondal PK, Pal I, Misra S, Biswas S, Bera SP (2009) Rhabdomyosarcoma of nose, nasopharynx and paranasal sinuses. Indian J Otolaryngol Head Neck Surg 61: 317–319. [View]
- Zhang Yanqiu, Li Peihua et al. (2010) Three cases of rhabdomyosarcoma of the nasal cavity and sinus [j]. Journal of Clinical Otorhinolaryngology Head and Neck Surgery 24: 524–525.
- Spunt SL, et al. Routine brain imaging is unwarranted in asymptomatic patients with rhabdomyosarcoma arising 0utside Of the head and neck region mat iS metadtatic at diagnosis: a report from the Intergroup RhabdomyoSarcoma Study Group [J]. Cancer,2001 92: 121–125.
- Guo Limin, Zhao Hui, et al. (2001) Clinical analysis of 17 cases of rhabdomyosarcoma of otolaryngology [j]. Journal of Clinical Otorhinolaryngology 15: 358–359. [View]
- GillesPie MB, et al. (2006) Pediatric Rhabdomyosarcoma of the Head and Neck. Current Treatment Options in Oncology 7: 13–22. [View]
- Wurm J, Constantinidis J, Grabenbauer GG, Iro H (2005) Rhabdomyosarcomas of the nose and paranasal sinuses: treatment results in 15 cases. Otolaryngol Head Neck Surg 133: 42–50. [View]
- Skubitz KM, D’Adamo DR (2007) Sarcoma. Mayo Clin Proc 82: 1409–1432. [View]
- Li Baozhong, Wu Yaohong, et al. (2005) Rhabdomyosarcoma of the head and neck (a report of 12 cases) [j]. Modern Oncology 13: 98–100.
- Wolfson A H, et al. (1998) Does a radiation dose response relation exist concerning survival of patients who have soft tissue sarcomas of the extremities: radiation dose relation for soft tissue sarcomas[J]. Am J Clin Oncol 2: 270–274.
- Huh WW, Skapek SX (2010) Childhood rhabdomyosarcoma: new insight on biology and treatment. Curr Oncol Rep 12: 402–410. [View]
- Ganjavi H, Gee M, Narendran A, et a1. (2005) Adenovirus-mediated p53 gene therapy in pediatric soft tissue sarcoma cell lines: sensitization to cisplatin and doxorubicin. Cancer Gene Ther 12: 397–406.
- Xiao Shaowen, Liu Changqing, Sun Yan, et al. (2007) Clinical observation of recombinant human p53 gene combined with radiotherapy and hyperthermia in the treatment of advanced soft tissue sarcoma. Chinese Journal of Clinical Oncology 34: 65–67.
- Wu TH, Huang JS. Wang HM, et al. (2010) Long-term survivors of adult rhabdomyosarcoma of maxillary sinus following multimodal therapy: case reports and literature reviews [J]. Chang Gung Med J 33: 466–447.