- 4192 Devonwood Way, Ashburn, Virginia, 20148
- Helpline: +1 (703) 665-3747
COVID-19 Pandemic Staffing at a Major Academic Medical Center
- Home
- Back to Journal
- Article Details
Stony Brook University Hospital (SBUH) is a 624-bed tertiary medical center located on Long Island, approximately 60 miles east of New York City. Our area has quickly become the epicenter of the COVID-19 pandemic, and on April 4th, New York State Governor, Andrew Cuomo, described the rapid spread of cases on Long Island as “a fire spreading”. To date, greater than 32,000 confirmed cases and over 1,000 deaths have been reported in our county by the end of April 2020 [1].
To meet the influx of patients, many of whom require an intensive care unit, the governor ordered hospitals in our region to submit a surge plan to increase beds by 50%. An expansion team was assembled which meets twice daily and has the authority to manage the opening and staffing of all new units, including the redeployment of personnel from every department. Along with the difficulties facing all hospitals in our region related to securing personal protective equipment, the shortage of ventilators and inadequate access to testing, the pandemic has also placed an enormous strain on the healthcare workforce.
Over a two-week period SBUH added 355 beds, doubling our ICU, step-down beds, and floor beds devoted to medical patients. We accomplished this by repurposing medical and surgical units, the Ambulatory Surgery Center, both the preoperative and postoperative units, the cardiac care center, and the outpatient cancer center. In addition, The Children’s Hospital and Pediatric Emergency Department began to care for patients up to age 30, including many COVID patients. Staffing all of these units required us to rethink our existing paradigms and utilize existing resources in new ways. This affected every level of our organization from attending and resident physicians to advanced practitioners and medical students.
First, we sought and were granted Pandemic Emergency Status from the Accreditation Council for Graduate Medical Education (ACGME). This allowed us to mobilize all of our residents and allowed our fellows to act as attendings in their core specialties. Residents from every program were classified with regard to their level of ICU experience then combined with our advanced practitioners to create clinically equivalent teams. These teams were then deployed to COVID-19 medical floors, step-down units, and intensive care units based on their clinical experience. ICU and step-down unit teams consisted of at least one ICU experienced member paired with a less experienced resident or advanced practitioner (Figure 1). Floor teams consisted of a medical resident paired with an off-service resident or advanced practitioner (Figure 1). We also recruited newly graduated medical students who were hired as “Assistant Attendings” and were paired with medical residents to staff non-ICU units.
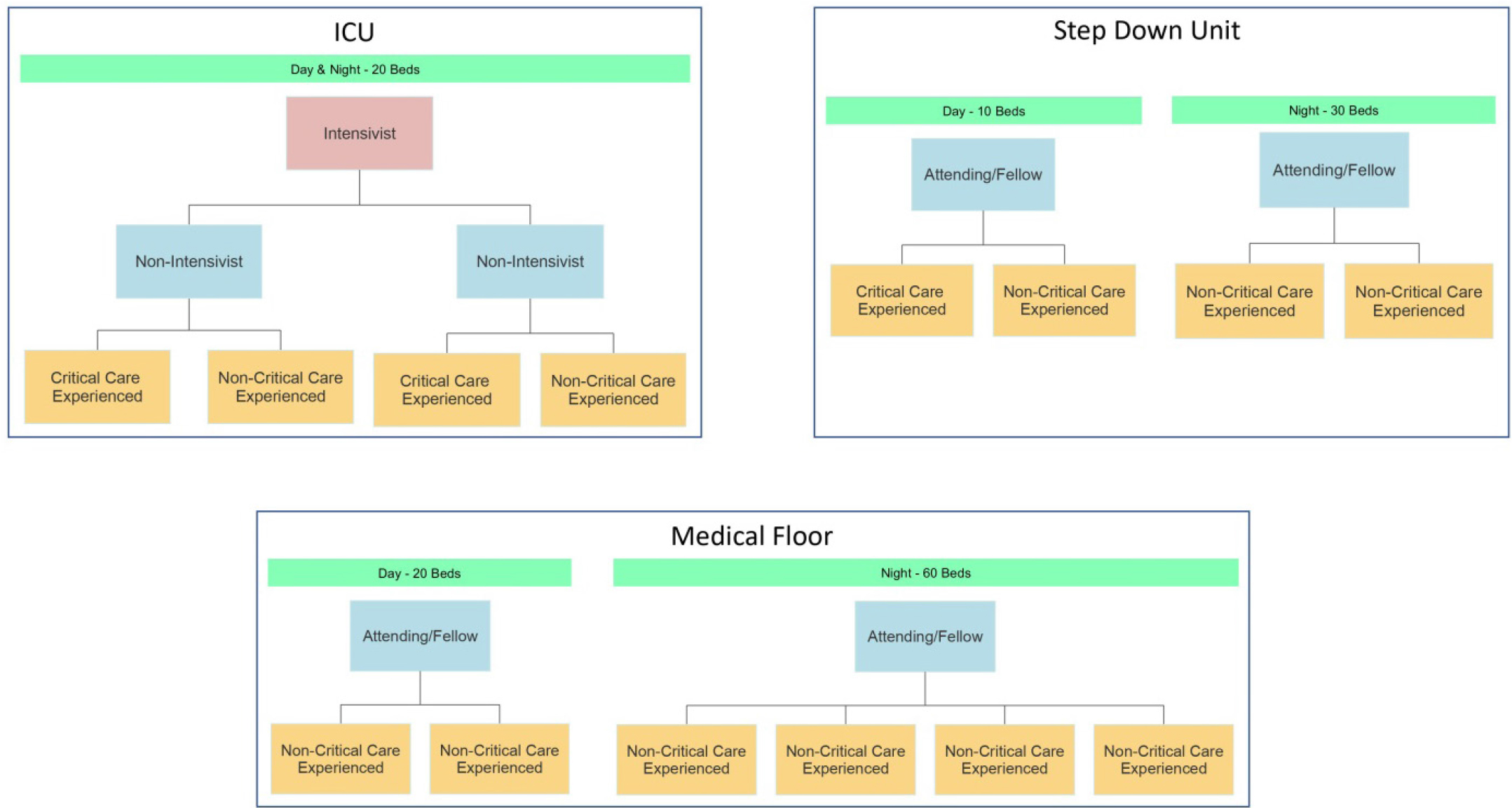
Figure 1: Physician and LIP staffing teams for the ICU, Step Down and Medical Units during COVID19.
Medical attendings and fellows from across the inpatient and outpatient services were recruited to supervise these teams. Educational material and COVID-19 clinical protocols were created and distributed to these providers to ensure patient safety. Additionally, each team has access to a dedicated Infectious Disease and Pulmonary specialist. The clinically equivalent teams of residents and advanced practitioners worked 5 days on and 5 days off whereas the attendings worked 7 on and 7 off. This schedule was chosen to help reduce physician fatigue and burnout particularly in the ICU setting where the care was quite intense. This overlapping coverage also allowed us to ensure continuity of care, which we found to be extremely important given the acuity of patients with COVID-19.
The severity of this disease has meant that the largest burden has fallen on our intensive care units. A completely new paradigm had to be created to safely manage the large influx of extremely sick patients. Each Intensivist supervised two clinical teams consisting of one non-intensivist attending or fellow with a clinically equivalent team. This arrangement allowed us to better utilize the knowledge and experience of our specialists while also ensuring direct attending supervision of each patient. Our surgical and medical intensivist directors also created clinical care standards and protocols to ensure that all patients received a similar level of same care. These documents have been updated frequently as we gain new experience, both from our international colleagues as well as from our own institution.
The deployment of residents and fellows required us to also rethink our non-COVID clinical services as well. With limited exceptions, each department re-worked schedules to cover the non-COVID surge services 24/7 with only attending physicians. This included cardiology, obstetrics, medical subspecialties, and others. Without the dedication of these attendings we would not have had the residents and advanced practitioners to populate our COVID services safely.
The rapid spread of this disease forced the entire hospital to react quickly and in unison to enact drastic but necessary changes to our everyday work patterns. Here we have presented the physician adaptations, but every department from facilities to procurement to nursing underwent similar transformations in response to SARS-CoV-2. We would like to thank every member of our healthcare team for their tireless efforts over the last several months to ensure that the people in our community received the best possible care in the most unprecedented of times. We hope that our experience will be an aid to any hospital unfortunate enough to suffer through a similar crisis.
Reference
- COVID-19 Case Update. April 2020. [View]